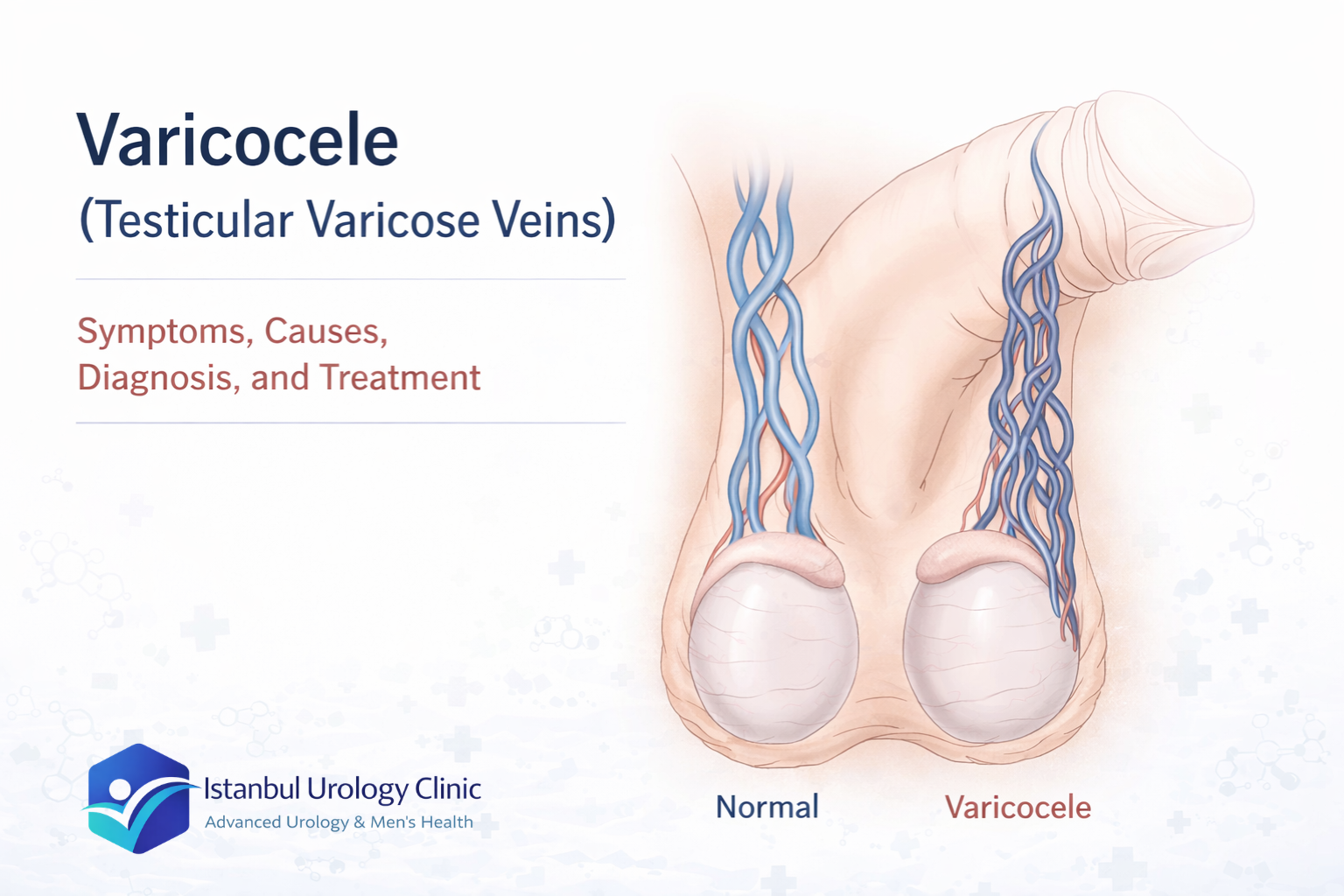
A varicocele is an abnormal enlargement of the veins inside the scrotum that drain blood away from the testicle.When those veins stop functioning correctly, blood pools inside them instead of moving efficiently upward.Over time, the pooling causes the veins to dilate and swell, creating the condition known as varicocele.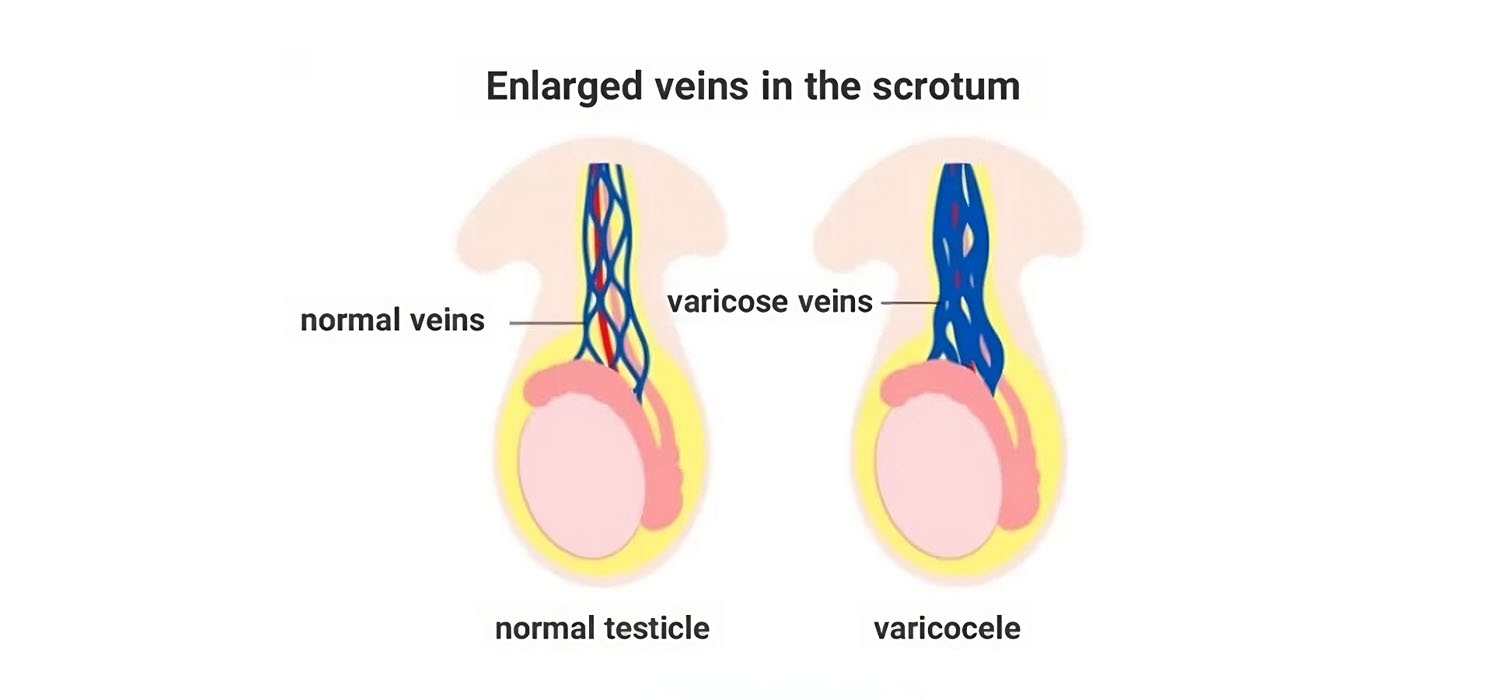 The mechanism is the same as varicose veins in the legs: blood collects, pressure builds, and the vessel wall stretches.In some men, the enlarged veins are visible or palpable through the scrotal skin.
The mechanism is the same as varicose veins in the legs: blood collects, pressure builds, and the vessel wall stretches.In some men, the enlarged veins are visible or palpable through the scrotal skin.
In others, they are small enough that only a Doppler ultrasound or physical examination by a urologist will detect them. Symptoms vary just as widely.
Many men with varicocele feel nothing at all. Others notice a dull heaviness in the testicle that builds through the day and is worse after prolonged standing. The next section covers why varicoceles develop and why some men are more prone to them than others.
Varicocele develops when the small one-way valves inside the testicular veins fail to do their job. These valves normally keep blood moving upward, away from the testicle and back toward the heart. When a valve weakens, blood reverses direction and begins to pool in the veins around the testicle. Over time, that pooling stretches the vein walls and produces the dilation that defines varicocele.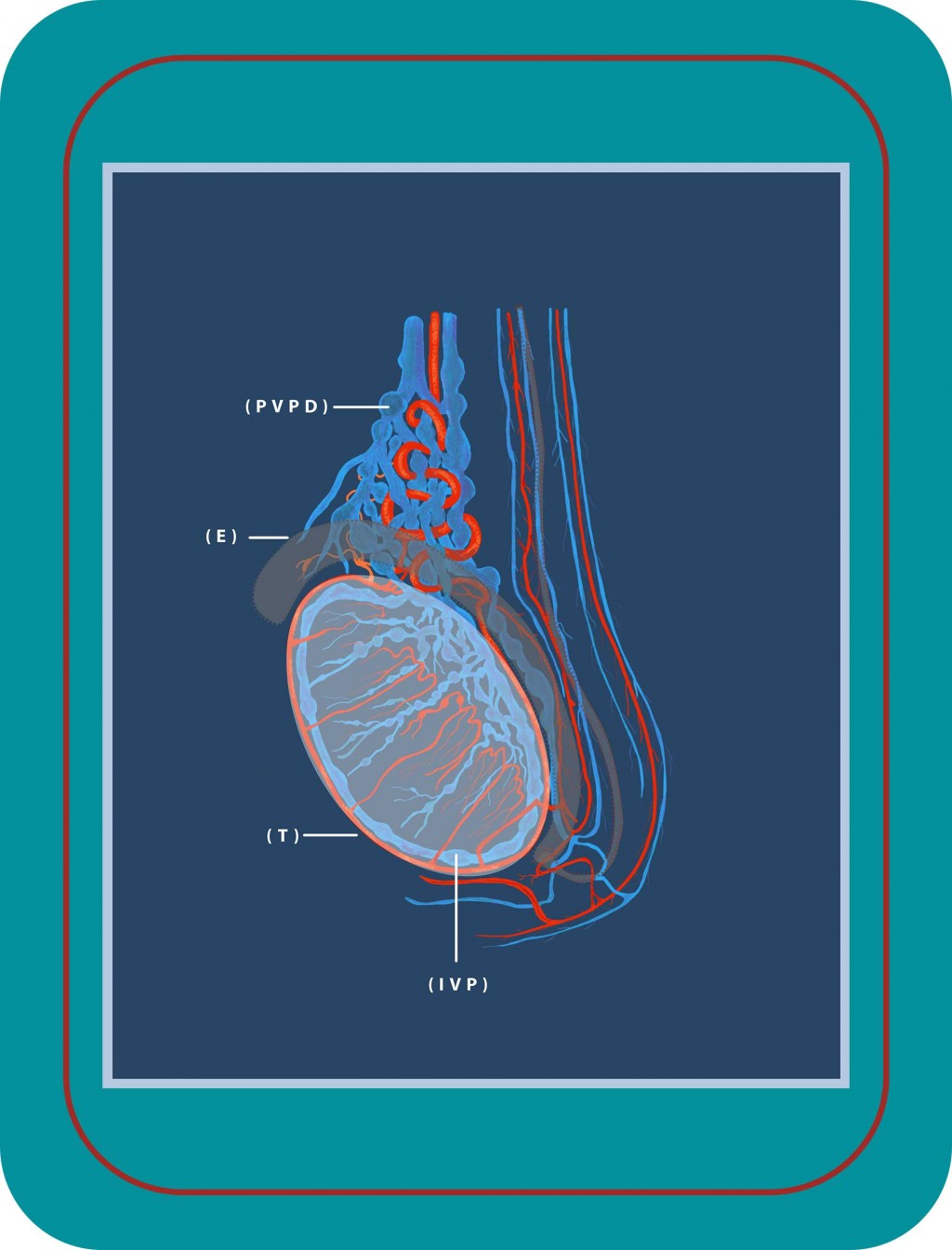
The mechanism is the same as varicose veins in the legs: blood collects, pressure builds, and the vessel wall stretches. The difference with varicocele is where it happens and why the left side is so disproportionately affected.
Why the Left Side Is Affected in 80 to 90% of Cases
Around 80 to 90% of varicoceles occur on the left side, and the reason comes down to anatomy.
The left testicular vein drains into the left renal vein at nearly a right angle. The right testicular vein, by contrast, drains directly into the inferior vena cava at a gentler angle and with lower resistance. That single difference in drainage geometry means blood has to work harder to leave the left testicle, and when valve function weakens, the left side is where pooling shows up first.
Bilateral varicocele (affecting both sides) is possible but less common. Isolated right-sided varicocele is uncommon enough that when it appears in an adult patient, it warrants additional investigation to rule out an underlying cause in the abdomen or kidney.
What Makes Varicocele More Likely
Two factors increase the chance of valve failure and venous pooling:
- Puberty and rapid growth. The testicles grow quickly during adolescence and blood flow to the area increases significantly. This is the period when most varicoceles first develop, and it is also why the condition is sometimes found incidentally during routine examinations in teenagers with no complaints.
- Increased abdominal pressure. Anything that raises pressure in the abdomen can compound the problem: chronic heavy lifting, prolonged standing, and certain occupations that involve sustained physical strain.
The condition is also frequently discovered during fertility investigations, since impaired testicular drainage affects the temperature and hormonal environment the testicle needs to produce healthy sperm.
When varicocele develops during adolescence, it can interfere with normal testicular growth. Blood pooling in the dilated veins raises the local temperature and disrupts the hormonal environment the developing testicle depends on.Over time, this can result in a measurable size difference between the two testicles, with the affected side growing more slowly or showing signs of reduced volume.
Blood pooling in the dilated veins raises the local temperature and disrupts the hormonal environment the developing testicle depends on.Over time, this can result in a measurable size difference between the two testicles, with the affected side growing more slowly or showing signs of reduced volume.
For this reason, varicocele diagnosed in teenagers is monitored carefully.Measuring testicular volume on both sides at regular intervals allows the urologist to track whether normal growth is continuing or whether the varicocele is having a progressive effect.
If a size difference begins to develop or worsens between appointments, treatment may be recommended to protect long-term testicular function before the damage becomes permanent.
Varicocele itself rarely causes severe or sudden symptoms.
But not every episode of testicular pain is varicocele, and some causes require immediate attention.
Seek medical evaluation without delay if you experience sudden or severe testicular pain, rapid swelling, or discomfort that escalates quickly.
These symptoms can indicate testicular torsion or acute infection, both of which require urgent treatment and cannot be managed by waiting.
The rule is straightforward: gradual, positional discomfort that has been present for days or weeks can be assessed at a scheduled appointment.
Sudden, severe, or rapidly worsening pain should be evaluated the same day.
Varicocele does not directly cause erectile dysfunction and does not interfere with sexual activity in the vast majority of men. Most men with varicocele have no noticeable impact on sexual performance, sometimes for decades without ever seeking treatment.The connection that does exist is indirect.
Most men with varicocele have no noticeable impact on sexual performance, sometimes for decades without ever seeking treatment.The connection that does exist is indirect.
When varicocele reduces testosterone production, some men notice a gradual decline in sexual desire or general energy levels.This is not the same as erectile dysfunction, and it is not universal.The primary concerns with varicocele are testicular discomfort and fertility.Sexual function is rarely the presenting problem, and it is rarely the reason treatment is recommended.
Both surgical repair and embolization close the enlarged veins responsible for blood pooling around the testicle.
The difference is in how those veins are reached and occluded.
In surgery, the surgeon accesses the veins directly through a small incision and ligates them under direct vision.
Blood is redirected away from the damaged veins and through healthy collateral channels.
Microsurgical varicocele repair uses magnification to identify and preserve the testicular artery and lymphatic vessels alongside the veins being treated.
This precision reduces the risk of recurrence and complications compared to conventional open surgery.
In embolization, no incision is made.
A thin catheter is guided through a peripheral vein, typically accessed from the groin or neck, and advanced to the affected testicular vein.
Blocking materials such as coils or sclerosing agents are deployed through the catheter to occlude the vein from within.
Embolization is minimally invasive and carries a shorter recovery time, but it is not available at all centres and may have slightly higher recurrence rates than microsurgical repair.
The choice between the two depends on which approach best suits the patient’s anatomy, clinical situation, and the expertise available.
No single treatment is right for every patient with varicocele.
The decision is shaped by three things: the severity of the varicocele, whether it is causing symptoms, and whether fertility is affected.
When No Treatment Is Needed
When none of those three factors apply, intervention is not indicated.
Regular monitoring is a legitimate and appropriate plan for mild, asymptomatic varicoceles with no fertility impact.
When Treatment Is Indicated
When persistent discomfort or abnormal semen parameters are present, treatment becomes the more appropriate path.
Microsurgical varicocelectomy is the preferred option in experienced centres.
The magnification it provides allows precise ligation of the affected veins while protecting the testicular artery and lymphatic vessels.
Minimally Invasive Alternative
Embolization is a viable catheter-based alternative that avoids surgical incision entirely.
It suits patients who prefer to avoid surgery or where the clinical situation makes a catheter-based approach more practical.
The final recommendation follows from the individual evaluation, not from a default protocol.